Congenital Anomalies
Developmental Alterations of Teeth
These alterations may be primary or arise secondary to environmental influences (e.g., concrescence, hypercementosis, and dilaceration).
Developmental Alterations of Teeth |
Number ➔ • Hypodontia ➔ • Hyperdontia ➔ Anodontia |
Size ● Microdontia ● Macrodontia |
Shape ➢ Gemination ➢ • Fusion ➢ • Concrescence ➢ • Accessory cusps ➢ • Dens invaginatus ➢ • Ectopic enamel ➢ • Taurodontism ➢ • Hypercementosis ➢ • Accessory roots ➢ • Dilaceration |
Structure ★ Amelogenesis imperfecta (AI) ★ • Dentinogenesis imperfecta (DGI) ★ • Dentin dysplasia type I (DD-I) ★ • Dentin dysplasia type II (DD-II) ★ • Regional odontodysplasia |
Number
Hypodontia

Hypodontia

Hypodontia: less than six missing teeth (not taking into account the third molars)
Oligodontia: six or more missing permanent teeth (not taking into account the third molars)
–
Anodontia: no teeth present
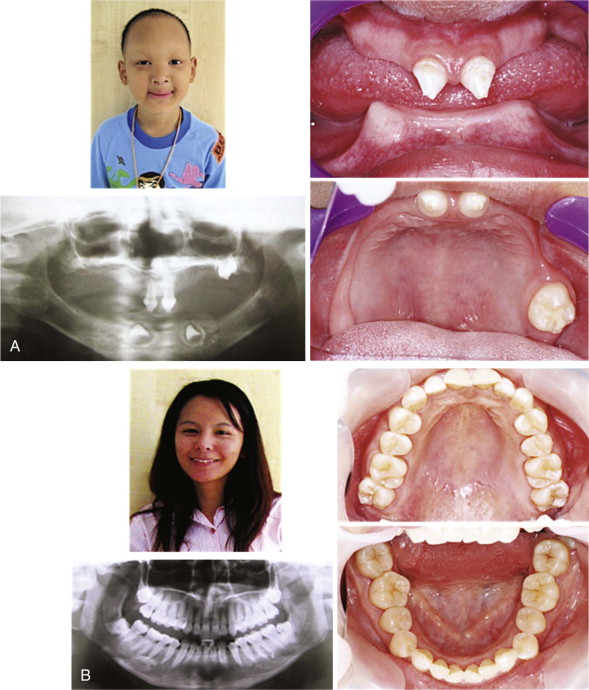
Hypodontia in a Thai boy.
Typical intra-oral and radiographic presentations in a boy with ectodermal dysplasia with multiple missing teeth; the teeth that are present are small and conical in shape. In the regions where teeth are absent, alveolar bone does not develop.
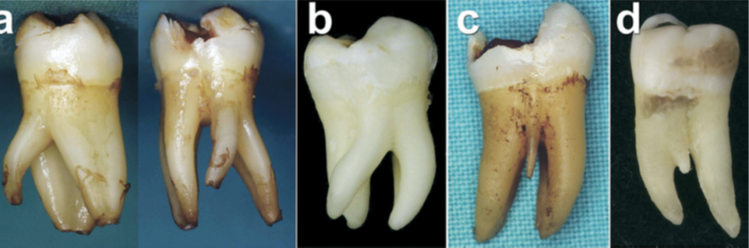
A, X-linked hypohidrotic ectodermal dysplasia caused by an EDA mutation. Note the severe hypodontia, sparse hair, and hyperpigmented skin around his eyes. B, His mother, who is heterozygous for the EDA mutation is phenotypically normal.

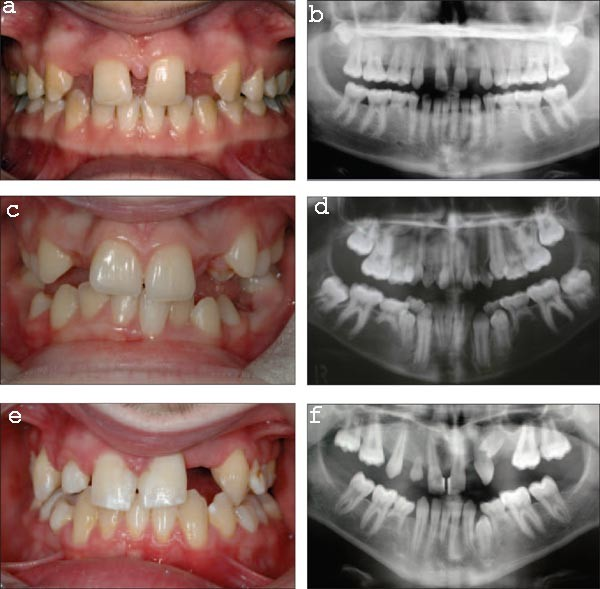
Conical primary teeth are often associated with missing permanent teeth. This child had an autosomal recessive form of ectodermal dysplasia and was missing almost all of the permanent teeth. (C) These teeth have been built up with composite resin strip crowns. (D) Radiographic appearance of the same child at 15 years of age. Most of the primary teeth have exfoliated even in the absence of a permanent successor. There has also been loss of bone in the region of the tuberosity due to pneumatization of the sinus that will complicate implant placement.
Frequency
Primary teeth |
~0.1–0.7% |
male : female |
ratio unknown |
Permanent teeth |
~2–9% |
male : female |
1 : 1.4 |
Third molars > maxillary lateral incisors > second premolars > mandibular central incisors.
Oligodontia/ anodontia is a major clinical feature :Major conditions manifesting
Dento-alveolar clefting. Trisomy 21 (Down syndrome). Chondroectodermal dysplasia (Ellis–van Creveld syndrome). Rieger syndrome. Incontinentia pigmenti. Oro-facial-digital syndrome Craniosynostosis syndromes. |
Hyperdontia
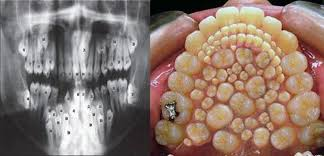

Syndromes associated with hyperdontia
These syndromes are all rare, but probably the best known is cleidocranial dysplasia


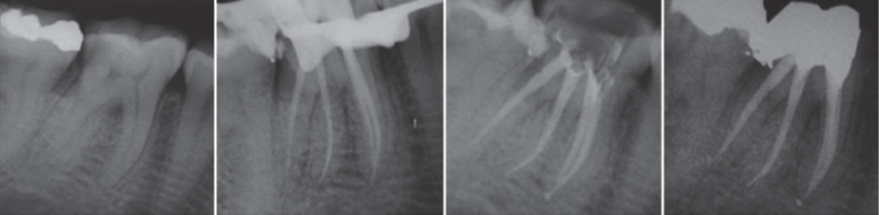
Radix Entomolaris and Paramolaris
Supernumery roots
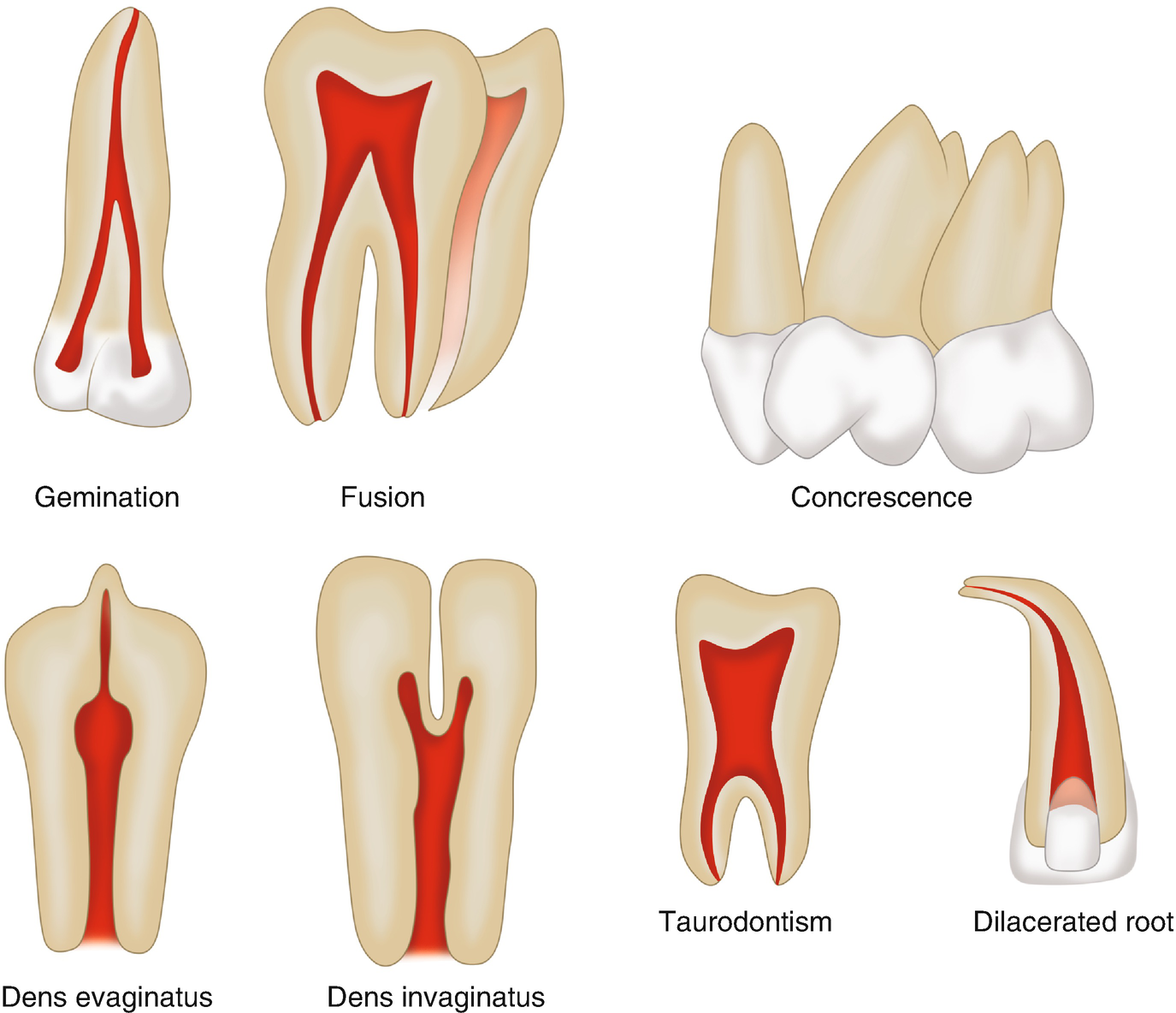
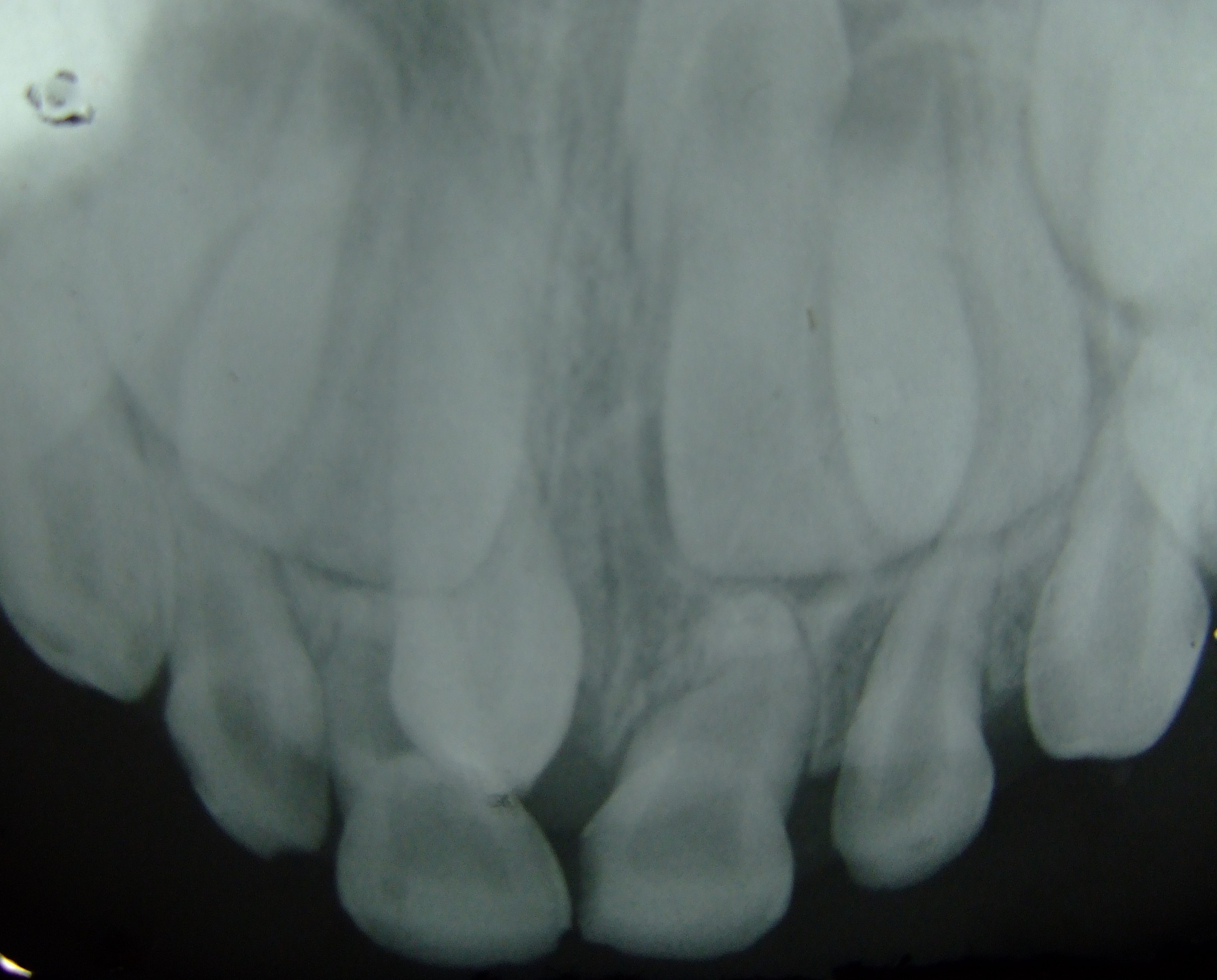
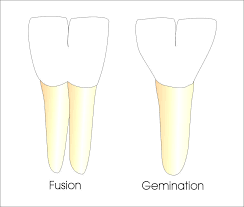
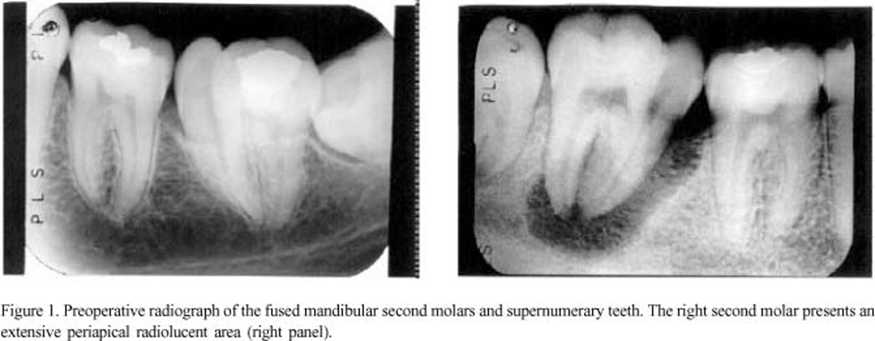
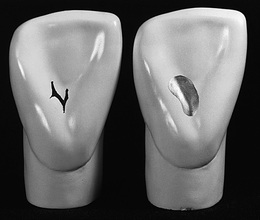
Gemination & Fusion

Gemination of a mandibular lateral incisor. The crown has a groove on the labial surface and is wider than normal.

Gemination: Teeth that are structurally united and have developed from the same tooth germ.
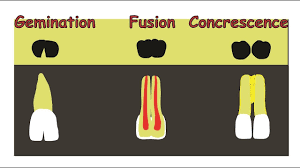
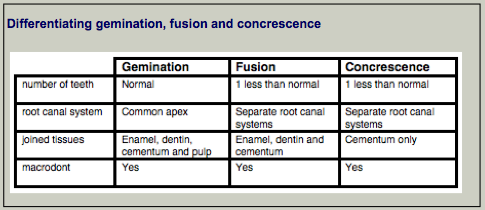


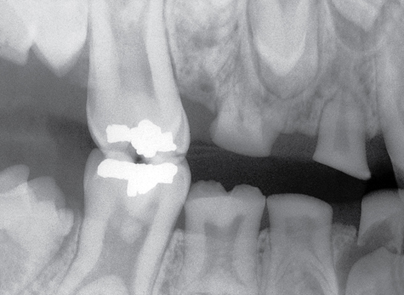
Concrescence


Two teeth during development or after they are completely formed, Joined with cementum
Common teeth are Posterior teeth
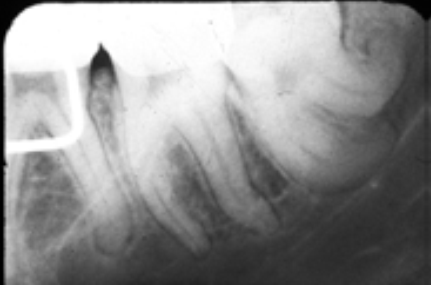
Taurodontism

Taurodontism is an apical extension of the pulp chamber that increases its apico-occlusal height and displaces the radicular bifurcation closer to the apex of a molar tooth.
Enamel pearls

Dilaceration
Dilaceration is an extraordinary curving or angulation of tooth roots.


Two developmental anomalies: Fusion and dilaceration
Dens Invaginatus & Evaginatus
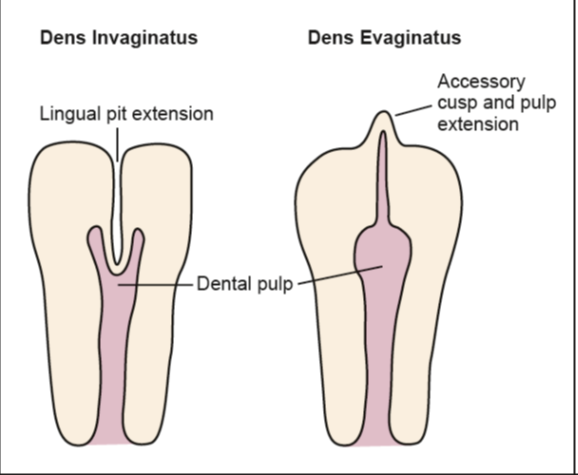
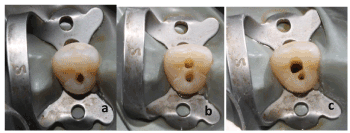
Dens Invaginatus (Dens-in-dente)

Invagination of a layer of enamel and dentin into pulp.


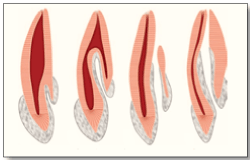
Oehlers’ classification of dens invaginatus
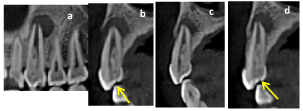

(a) and (b) clinical view showing the healing of the fistula 15 days after Calcium hydroxide dressing (c) a full thickness mucoperiosteal flap rising, exposing the apical lesion and a narrow root denudation (d) periapical pathologic tissues curettage and root end resection removing of the non sealed part of the canal (e) perfect apical sealing of biodentine orthograde obturation (f) post apical resection periapical radiograph
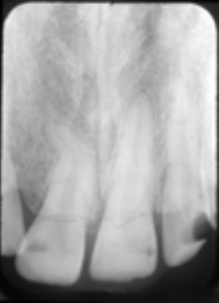
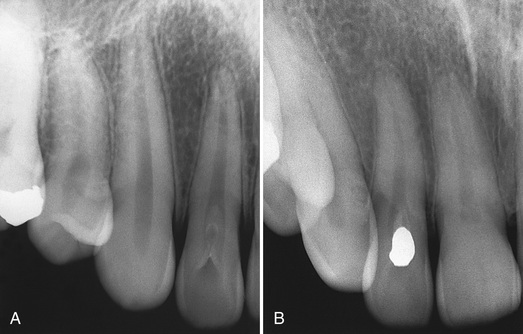
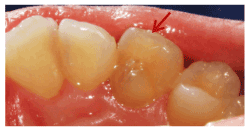
Lateral Incisor 12: Lingual Groove
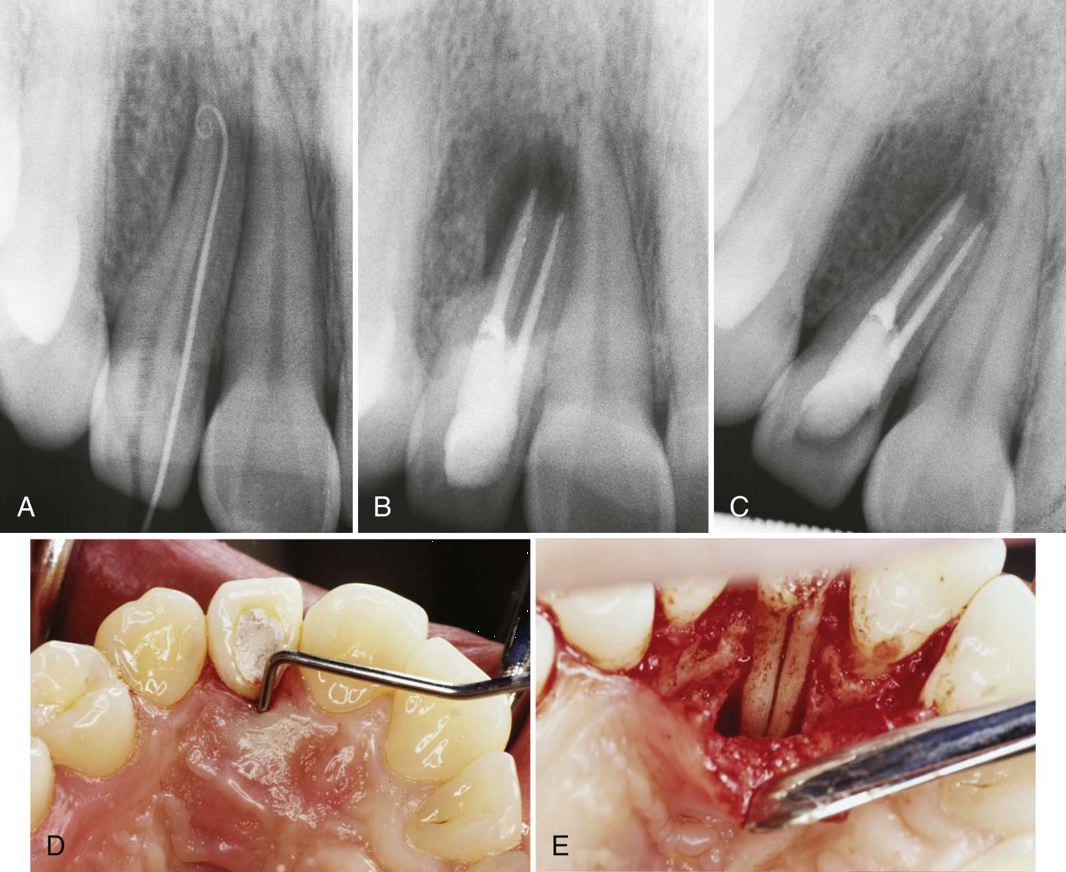
Case of developmental lingual groove causing primary endodontic infection. A, Preoperative radiograph of tooth 12. A gutta-percha marker extends to the apex. The radiograph is suggestive of a deep lingual groove or two separate roots. No caries or other abnormalities were present. B, A large lingual and periradicular defect developed after gutta-percha obturation of both canals (see photo in D). C, One-year recall after surgery showed radiographic healing, no symptoms, and a 3-mm probing depth. D, A 12-mm probing depth is demonstrated before surgical exploration. E, A large area of bone loss on the palatal and a deep lingual groove are evident during surgery

Dens Evaginatus
Developmental out folding of an enamel organ Usually on the occlusal surface of a premolar or a molar





talon cusp /dens evaginatus
Clinical significance
- If the cusp is small and asymptomatic, no treatment is required.
- If the cusp has deep developmental grooves which are non-carious, they should be cleaned and all the plaque and debris should be removed. After this they should be sealed with a fissure sealant or composite.
- If the grooves are decayed, the carious portion should be removed and the cavity has to be filled with glass ionomer cement or composite resin.
- If there is any occlusal interference, the cusp has to be reduced. The cusp may or may not contain vital pulp tissue. If a substantial portion of the cusp is to be reduced, it should be done conservatively followed by desensitizing agent application.
Structure
|
Amelogenesis imperfecta |
Dentinogenesis imperfecta |
Dentin |
Genetic |
Hypoplastic Hypomaturation Hypocalcified Chronological hypoplasia Molar-incisor hypomineralisation
|
Shell teeth
|
Dentinal dysplasia Regional odontodysplasia Multisystem disorders with associated dental defects Hypophosphatasia |
Infective |
Congenital syphilis |
|
|
Metabolic |
Rickets Hypoparathyroidism |
|
|
Other acquired developmental anomalies |
Fetal alcohol syndrome |
|
|
Drugs |
Tetracycline pigmentation Cytotoxic chemotherapy Fluorosis |
|
|
Hereditary Conditions of Teeth
|
Amelogenesis Imperfecta |
Dentinogenesis Imperfecta |
Dentin Dysplasia |
Heredity |
Many patterns |
Autosomal dominant |
Autosomal dominant |
Teeth affected |
All teeth, both dentitions |
All teeth, both dentitions |
All teeth, both dentitions |
Tooth color |
Yellow |
Yellow |
Normal |
Tooth shape |
Smaller, pitted |
Extreme occlusal wear |
Normal |
X-ray findings |
Normal pulps/dentin; reduced enamel |
Obliterated pulps, short roots, bell crowns |
Obliterated pulps, periapical cysts/granulomas |
Systemic manifestations |
No |
Osteogenesis imperfecta occasionally |
No |
Treatment |
Full crowns |
Full crowns |
None; early tooth loss |